Mohs micrographic surgery
Mohs surgery; Mohs MMS
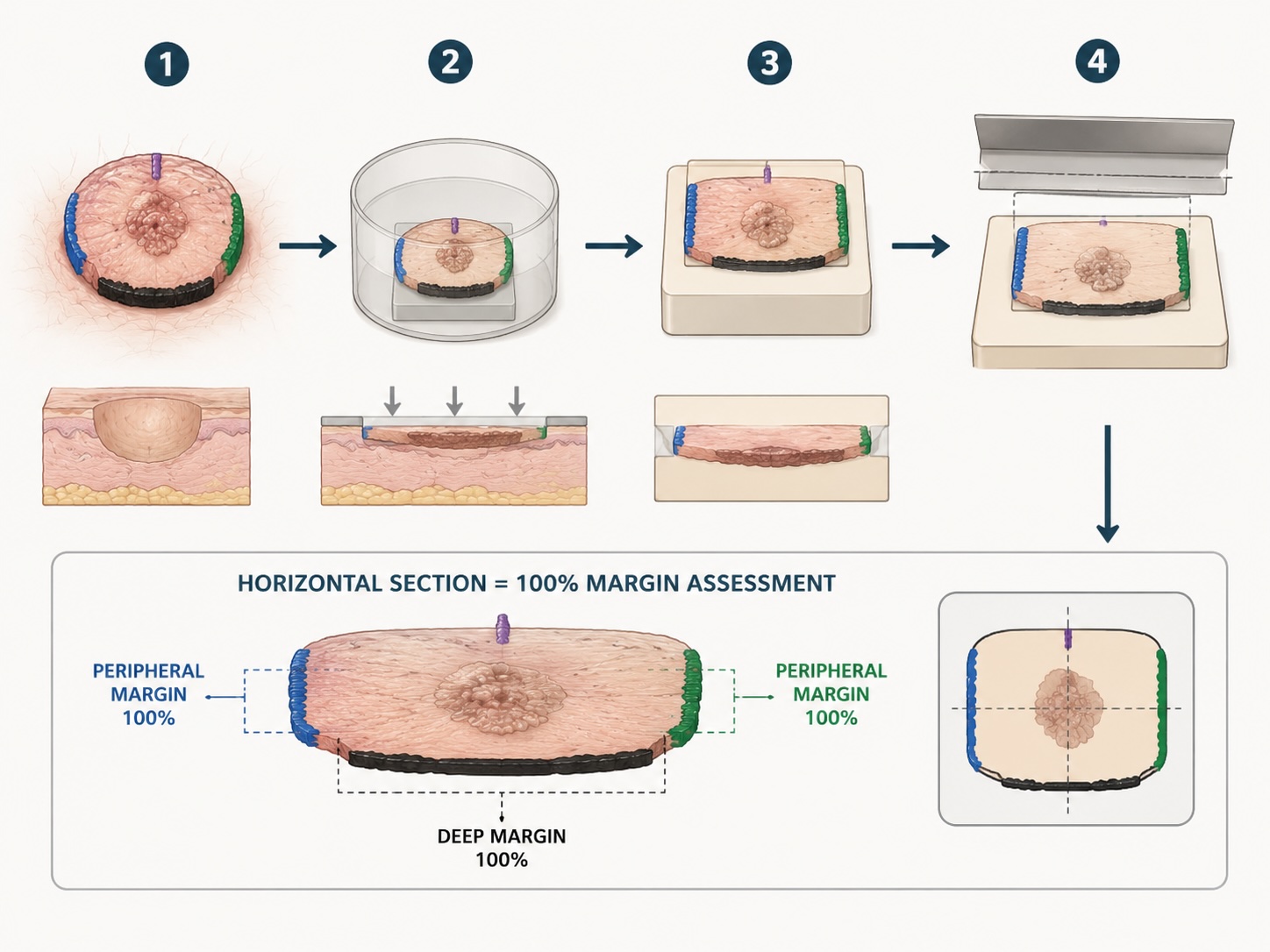
Mohs micrographic surgery is a tissue-sparing surgical technique with on-table frozen-section margin assessment of horizontally cut sections, allowing complete histological evaluation of 100% of the surgical margin. It offers the lowest recurrence rates for high-risk facial non-melanoma skin cancer and is the UK gold standard for selected BCC and cSCC.

Indications
BCC
- H-zone of the face (central face, periocular, nasolabial folds, ears).
- Recurrent BCC.
- Diameter >2 cm.
- High-risk histology — morphoeic, infiltrative, micronodular, basosquamous.
- Poorly defined clinical borders.
- Where maximal tissue sparing matters (eyelid, nasal ala, helix).
cSCC
- H-zone facial cSCC.
- Recurrent cSCC.
- BWH T2b. (BWH T3 — bone invasion, ≥ 4 risk factors or otherwise advanced disease — generally requires staging imaging plus composite resection and MDT discussion (± adjuvant radiotherapy) rather than Mohs.)
- Immunosuppressed patients (OTR, CLL).
- Perineural invasion present (in addition to wide margin).
Other
- Lentigo maligna — frozen-section Mohs with MART-1 / SOX10 immunostaining (specialist centres).
- DFSP — Mohs with CD34 IHC reduces recurrence vs wide local excision.
- Sebaceous carcinoma (periocular).
- Microcystic adnexal carcinoma.
- Atypical fibroxanthoma.
Technique
- Mark the visible tumour with a 1–2 mm clinical margin and orientation marks (often 12 o'clock).
- Excise stage 1 — disc of skin removed at a 45° bevel, en bloc with the underlying soft tissue. Specimen marked with tissue dye for orientation, divided into segments, mapped on a Mohs map.
- Frozen section — segments are flattened onto glass for horizontal cryosectioning. The surgeon (or pathologist) reads the entire deep and peripheral margin in one slide per segment.
- Map positive margins back to the patient using the Mohs map and excise only the area with residual tumour (stage 2). Repeat.
- Reconstruct when clear margins confirmed — usually same-day.
Evidence
The strongest evidence comes from the Dutch RCT of Mohs vs standard surgical excision for facial BCC (van Loo 2014). For primary BCC there is a modest absolute benefit; for recurrent BCC the benefit is larger (~10 percentage points difference in recurrence at 10 years).
- 10-year recurrence: primary BCC ~4% (Mohs) vs ~12% (standard).
- 10-year recurrence: recurrent BCC ~4% (Mohs) vs ~14% (standard).
- cSCC: Mohs reduces 5-year recurrence in high-risk subtypes vs standard excision (observational evidence).
UK availability and pathway
Mohs services in the UK are provided by accredited Mohs centres (most major teaching hospitals; some private). Referral pathways vary by Cancer Alliance — typically through the local skin cancer MDT. Demand often exceeds capacity; lead times of 6–12 weeks are common.
British Society for Dermatological Surgery (BSDS) maintains accreditation criteria for Mohs surgeons in the UK.
When Mohs is not available
- Wide local excision with appropriate margin and paraffin-embedded margin assessment ('staged excision' if delayed reconstruction).
- 2-stage 'square procedure' with paraffin permanent sections of the entire peripheral margin (alternative to Mohs for lentigo maligna).
- Definitive radiotherapy where surgery not feasible.
Complications
- Bleeding, infection, scar.
- Nerve injury (specific to anatomical site).
- Aesthetic morbidity from tissue loss.
- Long operative time for multi-stage cases.
- Anxiety / fatigue for patient through multiple stages.
References
- van Loo E et al. Surgical excision versus Mohs micrographic surgery for basal cell carcinoma of the face: 10-year follow-up. Eur J Cancer; 2014.
- British Society for Dermatological Surgery. UK Mohs surgery accreditation standards.
- Connolly SM et al. AAD/ACMS/ASDSA/ASMS 2012 appropriate use criteria for Mohs micrographic surgery. J Am Acad Dermatol; 2012;67:531–50.
Spot a correction?
If any clinical statement, citation or link on this page needs updating, please email admin@skinoncology.net with the page name, the proposed correction and the supporting source.