Cutaneous squamous cell carcinoma
Synonyms: cSCC; SCC of skin; squamous cell carcinoma of skin
Cutaneous SCC is the second-commonest skin cancer and accounts for the majority of non-melanoma skin cancer mortality. Risk stratification — particularly the Brigham & Women's (BWH) T-stage — drives margin choice, the case for adjuvant radiotherapy, and surveillance intensity. In solid organ transplant recipients, published cohorts report cSCC incidence roughly 65–100× higher than the general population, varying by organ, geography, immunosuppression and time from transplant.


What is cutaneous SCC?
cSCC is a malignant tumour of keratinocytes that invades the dermis. It usually arises from a precursor lesion (actinic keratosis or Bowen's disease) on chronically sun-damaged skin, but de novo cSCC occurs in scars, sinuses, chronic ulcers (Marjolin's), at HPV-associated sites and after radiotherapy.
Who gets cSCC?
UK incidence exceeds 50,000 cases per year. Predominantly head and neck of older patients with chronic UV exposure. Solid organ transplant recipients (OTRs) carry markedly increased cSCC risk, commonly quoted around 65–100-fold in published cohorts; cSCC can outnumber BCC in long-term renal transplant recipients.
Risk factors
- ☀Chronic UVOutdoor occupation; cumulative dose; Fitzpatrick I–II.
- ●Pre-malignantAK, Bowen's disease, and anogenital lichen sclerosus (the lichen sclerosus — cSCC association is predominantly at vulval / penile / perianal sites).
- ⊘ImmunosuppressionOTRs (esp. AZA), CLL, biologics, voriconazole.
- ⌐Chronic woundsMarjolin's ulcer in burns, sinuses, hidradenitis.
- ☢Prior RTLatency 10–30 years.
- VHPVPeriungual, genital, EV-associated.
- XXP, EVXeroderma pigmentosum; epidermodysplasia verruciformis.
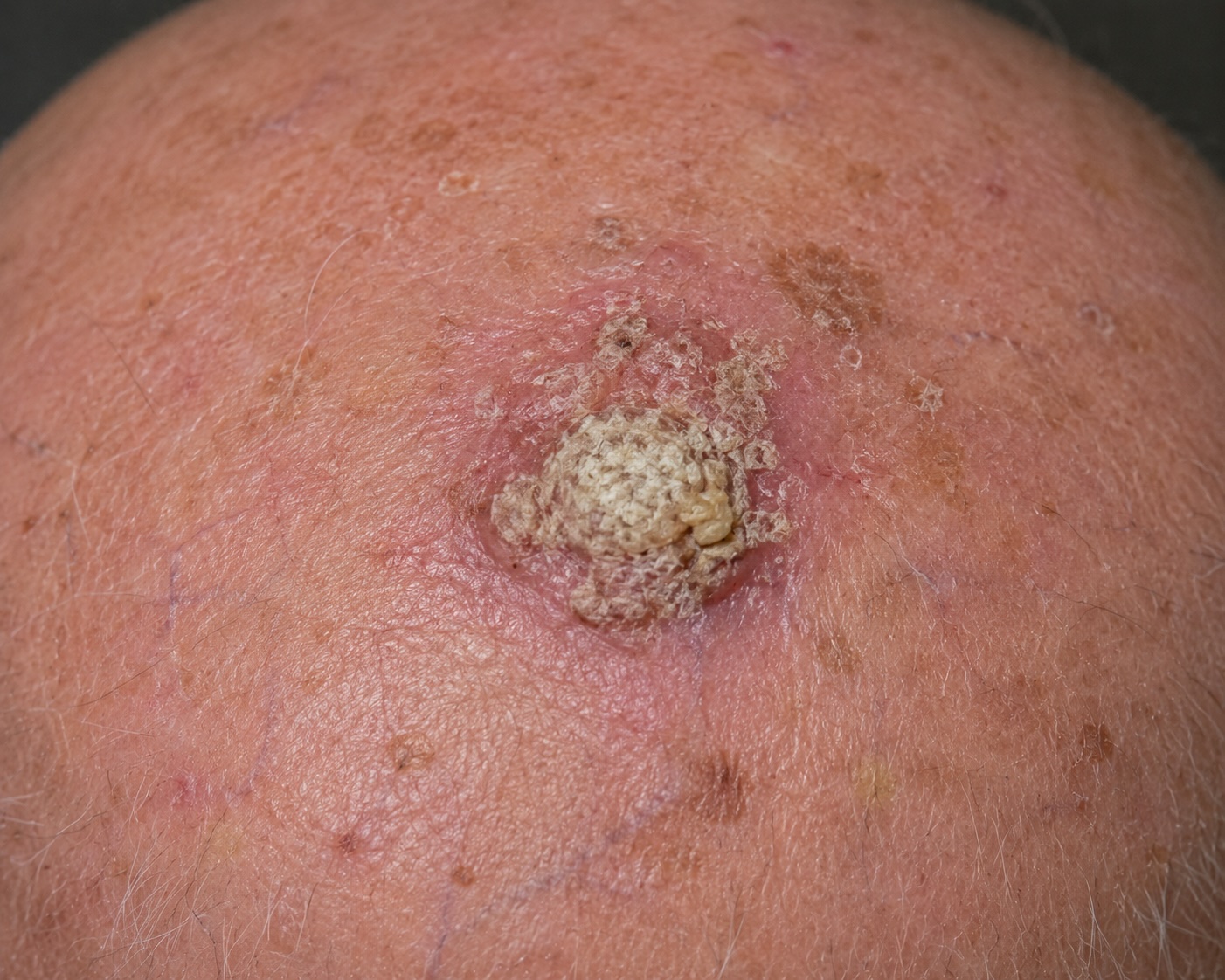
Clinical features
Typical presentations:
- Hyperkeratotic plaque or nodule on chronically sun-damaged skin — face, scalp, dorsal hand, forearm, helix, lip.
- Crusted papule with surrounding erythema; may bleed when traumatised.
- Cutaneous horn with broad indurated base — cSCC must be excluded.
- Non-healing ulcer >6 weeks — biopsy.
- Rapidly growing nodule — keratoacanthoma vs cSCC differential (often histologically inseparable).

Dermoscopy
- Polymorphous (mixed dotted and linear-irregular) vessels.
- White circles around hair follicles ('targetoid').
- Keratin / scale; central ulceration.
- White structureless areas (keratinisation).
- Glomerular vessels are characteristic of Bowen's (in-situ cSCC).
Risk stratification
Risk stratification should use the Brigham & Women's (BWH) T-stage in parallel with clinical high-risk features. Use the interactive BWH staging tool.
BWH risk factors
- Tumour diameter ≥2 cm.
- Poor differentiation.
- High-risk perineural invasion — the BWH PNI risk factor is nerve calibre ≥ 0.1 mm ONLY. PNI of a named nerve and tumour invasion beyond / deeper than the dermis (or of a deep nerve) are separate AJCC 8 / TNM 8 high-risk descriptors, not the BWH calibre factor.
- Invasion beyond subcutaneous fat.
- Bone invasion → automatic T3.
BWH T-stage
| Stage | Risk factors | Cohort-level nodal mets | Cohort-level death of disease |
|---|---|---|---|
| T1 | 0 | <1% | ~0% |
| T2a | 1 | ~5% | ~1% |
| T2b | 2–3 | ~20% | ~10% |
| T3 | 4 or bone invasion | >50% | >30% |
The percentages are approximate cohort-level estimates from BWH derivation / validation studies, not individual predictions; T3 denominators are small. BWH T2b and T3 cSCC should prompt imaging for nodal and distant disease, MDT discussion, and consideration of Mohs, adjuvant radiotherapy and systemic therapy.
Ultrasound of the nodal basin is a low-threshold first investigation for large or high-risk cSCC. CT neck/chest or MRI (for suspected PNI) is indicated in BWH T2b / T3 disease per MDT.
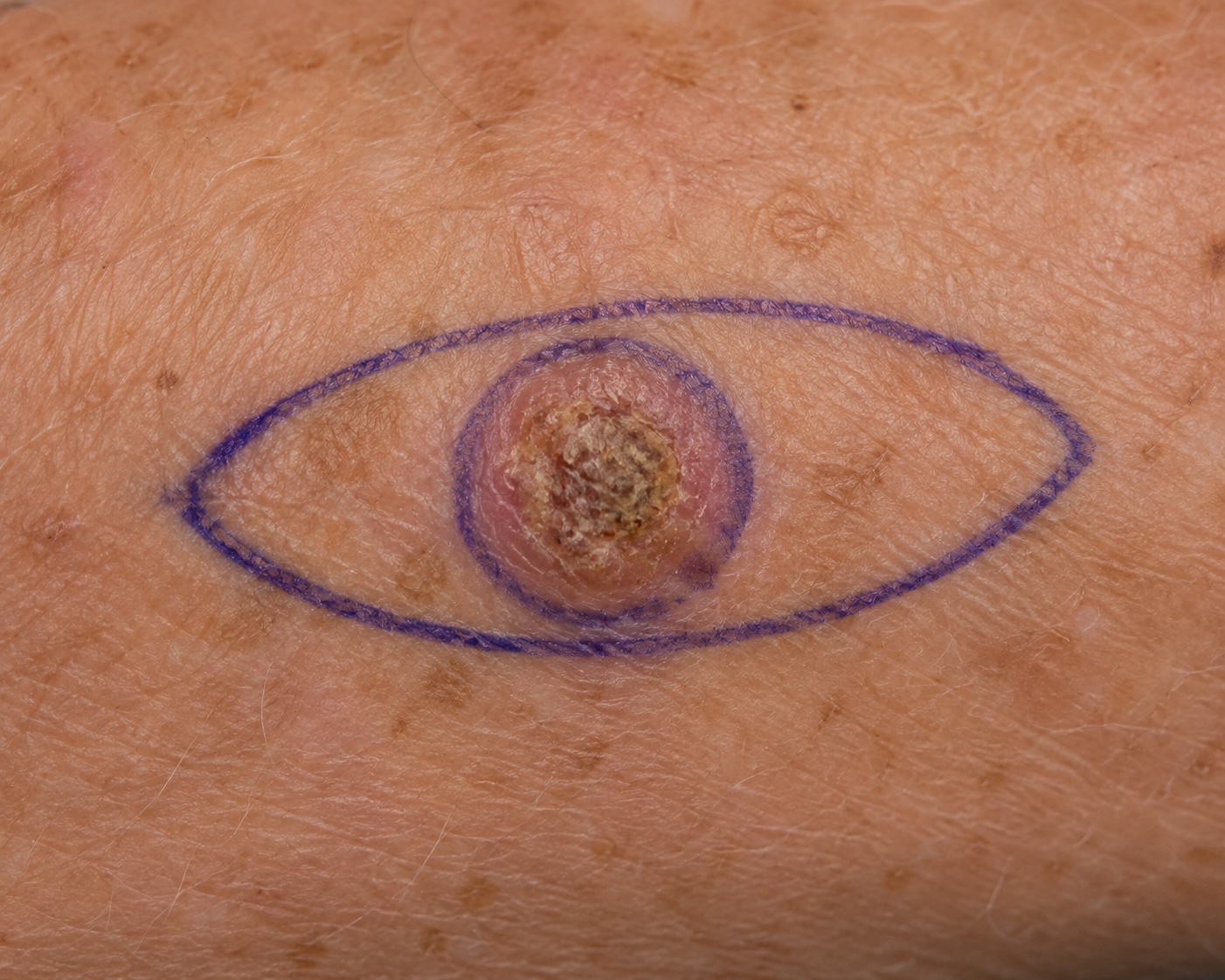
Management
Guideline Surgical margins (BAD 2020)
| Risk | Peripheral margin |
|---|---|
| Low-risk (<2 cm, well-diff, no PNI, depth <6 mm, body site, non-immunosuppressed) | 4 mm |
| High-risk (any feature above) | 6–10 mm or Mohs |
Mohs micrographic surgery
See Mohs technique reference. Indicated for H-zone cSCC, recurrent disease, poorly defined borders, >2 cm on face, immunosuppression, or where maximal tissue sparing is needed.
Adjuvant radiotherapy
Indication is largely Local MDT-driven; the bullets below are the consensus indications used at most UK centres.
- Consensus High-risk perineural invasion — PNI of a named nerve, radiologically detected perineural spread, or extensive PNI (multiple nerves involved or PNI of nerves with calibre ≥ 0.1 mm and/or beyond the dermis where the risk of in-transit perineural spread is appreciable).
- Local MDT Close or positive margin where further surgery is not feasible.
- Consensus Multiple involved nodes; extracapsular spread.
- Local MDT Recurrent disease.
Systemic therapy
- NICE TA Cemiplimab (anti-PD-1) — NICE TA802, first-line for advanced cSCC. Durable responses in ~50%.
- In development Pembrolizumab — NICE appraisal in development for adjuvant locally advanced cSCC after surgery and radiotherapy; no final NICE TA at last verification. Current NICE-approved systemic option for advanced cSCC is cemiplimab (TA802).
- Consensus Cetuximab; cisplatin ± 5-FU — historic options where ICI contraindicated.
- Local MDT Caution with ICI in OTRs — graft rejection risk; transplant team co-decision essential.
cSCC in immunosuppressed patients
OTRs warrant distinct management. See dedicated monograph.
- Annual (or more frequent) total-body skin examination from transplant onwards.
- Field-change treatment (5-FU, imiquimod, MAL-PDT).
- Early excision of any cSCC — no watch-and-wait.
- Acitretin chemoprophylaxis (0.2–0.5 mg/kg/day) where cSCC burden accelerates.
- Calcineurin-inhibitor → mTOR inhibitor conversion (sirolimus, everolimus) reduces incidence.
- Minimise voriconazole.
- Dedicated transplant dermatology clinic where available.
Follow-up
- Low-risk: single post-treatment appointment where appropriate to check histology, examine skin and nodes, provide education and safety-netting; then discharge.
- High-risk: 4-monthly for 12 months, then 6-monthly for a further 12 months; discharge at 2 years if stable and no overriding risk of further high-risk primaries.
- Very high-risk: 4-monthly for 24 months, then 6-monthly for a further 12 months; discharge at 3 years if stable and no overriding risk of further high-risk primaries.
- Metastatic cSCC after treatment: 3-monthly for 24 months, then 6-monthly for a further 36 months; consider longer-term review depending on patient and tumour factors.
- Immunosuppressed / OTR: apply the index-tumour risk schedule and keep high-risk patients under lifelong whole-skin surveillance at an MDT / transplant-dermatology agreed interval.
Prognosis
Most cSCC is cured by simple excision. Mortality is concentrated in high-risk disease — BWH T2b/T3, head and neck, immunosuppressed, recurrent. Five-year disease-specific survival is approximately:
- Low-risk: >99%.
- BWH T2a: ~95%.
- BWH T2b: ~80–90%.
- BWH T3: ~60%.
- Metastatic (pre-cemiplimab): <30%; substantially improved with ICI.
References
- Keohane SG et al. British Association of Dermatologists guidelines for the management of people with cutaneous squamous cell carcinoma 2020. Br J Dermatol. 2021;184(3):401-414.
- Jambusaria-Pahlajani A et al. Brigham & Women's T-stage for cSCC. JAMA Dermatol; 2013;149:402–10.
- Migden MR et al. PD-1 blockade with cemiplimab in advanced cSCC. N Engl J Med; 2018.
- NICE. Cemiplimab for treating advanced cutaneous squamous cell carcinoma (TA802). Published 29 June 2022 (replaced TA592, 2019 Cancer Drugs Fund interim guidance).
- Royal College of Pathologists. Dataset for histopathological reporting of primary invasive cutaneous squamous cell carcinoma and regional lymph nodes (G124). London: RCPath; February 2019; updated appendices available via the RCPath cancer datasets hub.
Spot a correction?
If any clinical statement, citation or link on this page needs updating, please email admin@skinoncology.net with the page name, the proposed correction and the supporting source.