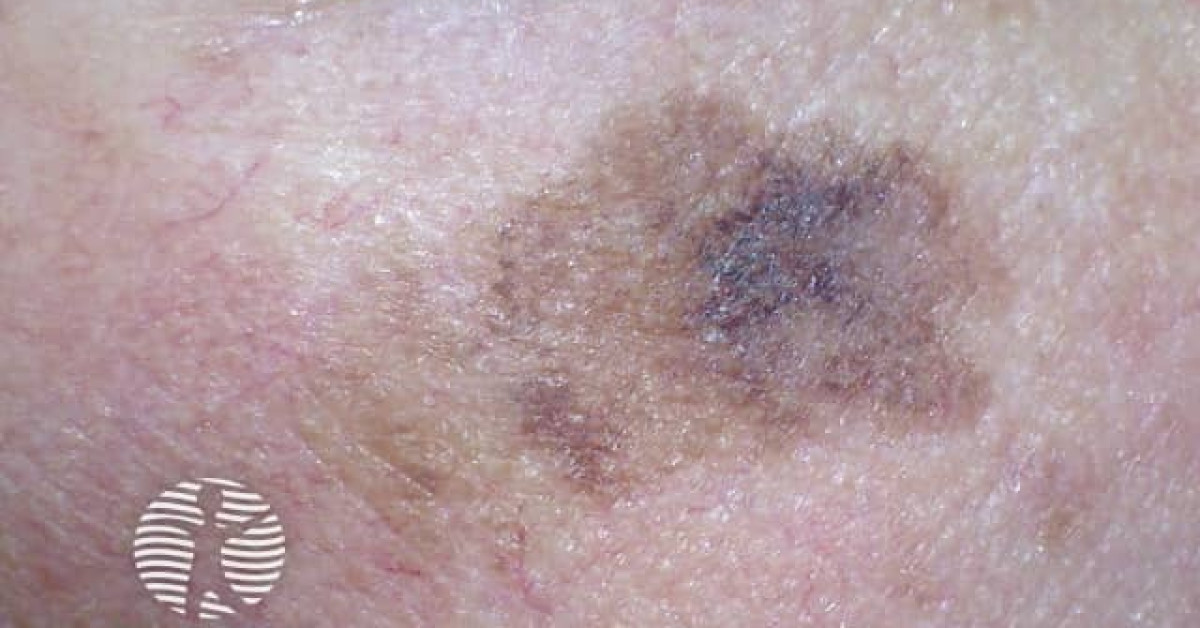
Lentigo maligna
Hutchinson's melanotic freckle; LM; melanoma in situ, lentigo maligna type
Melanoma in situ occurring on chronically sun-damaged skin, typically the face of older patients. Subclinical extension is common; staged excision, Mohs with melanocytic immunostaining and imiquimod are the principal treatment options.
Management
Staged ('slow Mohs') excision
Peripheral margin 5–10 mm (NICE NG14 in-situ margin; the wider end is commonly used for LM given subclinical extension), with 5 mm a common initial staged increment; square or rectangular excision with paraffin-embedded peripheral margin assessment, often over several stages, until clear margins are achieved. Reconstruction delayed until clearance confirmed.
Mohs with immunostains
Frozen-section Mohs with MART-1 / SOX10 / MITF is equivalent to staged excision in expert hands with same-day reconstruction.
Imiquimod
Imiquimod 5% daily or 5×/week for 8–12 weeks, under dermatology supervision, is an option for patients unsuitable for surgery; cure rates 60–80%, inferior to surgery.
Radiotherapy
Definitive radiotherapy (superficial / kilovoltage soft X-ray therapy) is an option where surgery is declined or unsuitable; outcomes comparable in selected series.
Before committing to a non-surgical strategy, ensure multiple representative biopsies have excluded an invasive component — broad shave or multiple 4 mm punches across the lesion, not a single central biopsy.
References
- NICE NG14. Melanoma: assessment and management. London: NICE; 2015 (last updated 27 July 2022).
Spot a correction?
If any clinical statement, citation or link on this page needs updating, please email admin@skinoncology.net with the page name, the proposed correction and the supporting source.