Cutaneous melanoma
Synonyms: malignant melanoma; melanoma of skin; MM
Cutaneous melanoma is a malignant tumour of melanocytes responsible for the majority of UK skin cancer deaths. Management is stage-directed, multidisciplinary and rapidly evolving with adjuvant and metastatic immune checkpoint inhibitors. Early diagnosis transforms outcomes — most patients with thin melanoma are cured by simple wide local excision.

What is cutaneous melanoma?
Cutaneous melanoma is a malignant proliferation of melanocytes — the pigment-producing cells of the basal epidermis. Melanocytes acquire genetic damage (predominantly UV-driven) and lose normal growth controls, producing first an in-situ or 'radial' growth phase and then in many subtypes a 'vertical' growth phase with capacity to metastasise.
Melanoma represents fewer than 5% of UK skin cancers but causes the majority of skin cancer deaths. Outcomes are starkly stage-dependent — a patient with a thin melanoma (Breslow ≤ 1 mm) has >95% five-year survival, while metastatic melanoma five-year survival was once below 10%, but is now 30–60% in selected patients on contemporary immunotherapy.
Who gets melanoma?
Cutaneous melanoma is the fifth commonest cancer in the UK, with around 17,500 new cases per year (NCRAS rolling average) and approximately 2,300 annual deaths. Incidence has more than doubled since the 1990s. Median age at diagnosis is in the seventh decade, but melanoma is the most common cancer in UK adults aged 25–29.
Risk factors
- ☀UV exposureIntermittent intense UV (sunburn) and chronic UV. Sunbeds are an IARC Class I carcinogen.
- IFitzpatrick I–IIFair skin, red or blonde hair, blue or green eyes; freckling; childhood sunburn.
- ●Naevi≥100 common naevi; ≥5 atypical naevi; large congenital melanocytic naevus.
- ⌂Family historyFAMMM / CDKN2A; CDK4; BAP1; POT1 mutations.
- ♥Personal historyPrior melanoma confers ~10× risk of a second primary.
- ⊘ImmunosuppressionOTRs 2–3× incidence; HIV; immune-modulating drugs.
- DDNA-repair syndromesXeroderma pigmentosum; some Lynch variants.
- ⚥Anatomy by sexTrunk in men; lower limb in women.
What causes melanoma?
Accumulated genetic damage in melanocytes drives uncontrolled proliferation and loss of apoptosis. UV radiation is the dominant environmental driver in superficial spreading and lentigo maligna melanomas; non-UV pathways predominate in acral lentiginous, mucosal and uveal subtypes.
Driver mutations and pathway groupings (Bastian framework)
| Pathway | Common drivers | Typical subtype |
|---|---|---|
| Intermittent UV (low CSD) | BRAF V600E/K (≈50%); NRAS (15–20%) | Superficial spreading |
| Chronic UV (high CSD) | NRAS, NF1, KIT | Lentigo maligna melanoma |
| Acral / mucosal | KIT, NRAS, BRAF (variable) | Acral lentiginous; mucosal |
| Uveal | GNAQ, GNA11, BAP1 | Uveal melanoma |
| Naevus / spitzoid | HRAS, kinase fusions (ALK, ROS1, NTRK) | Spitz melanoma |
Clinical features
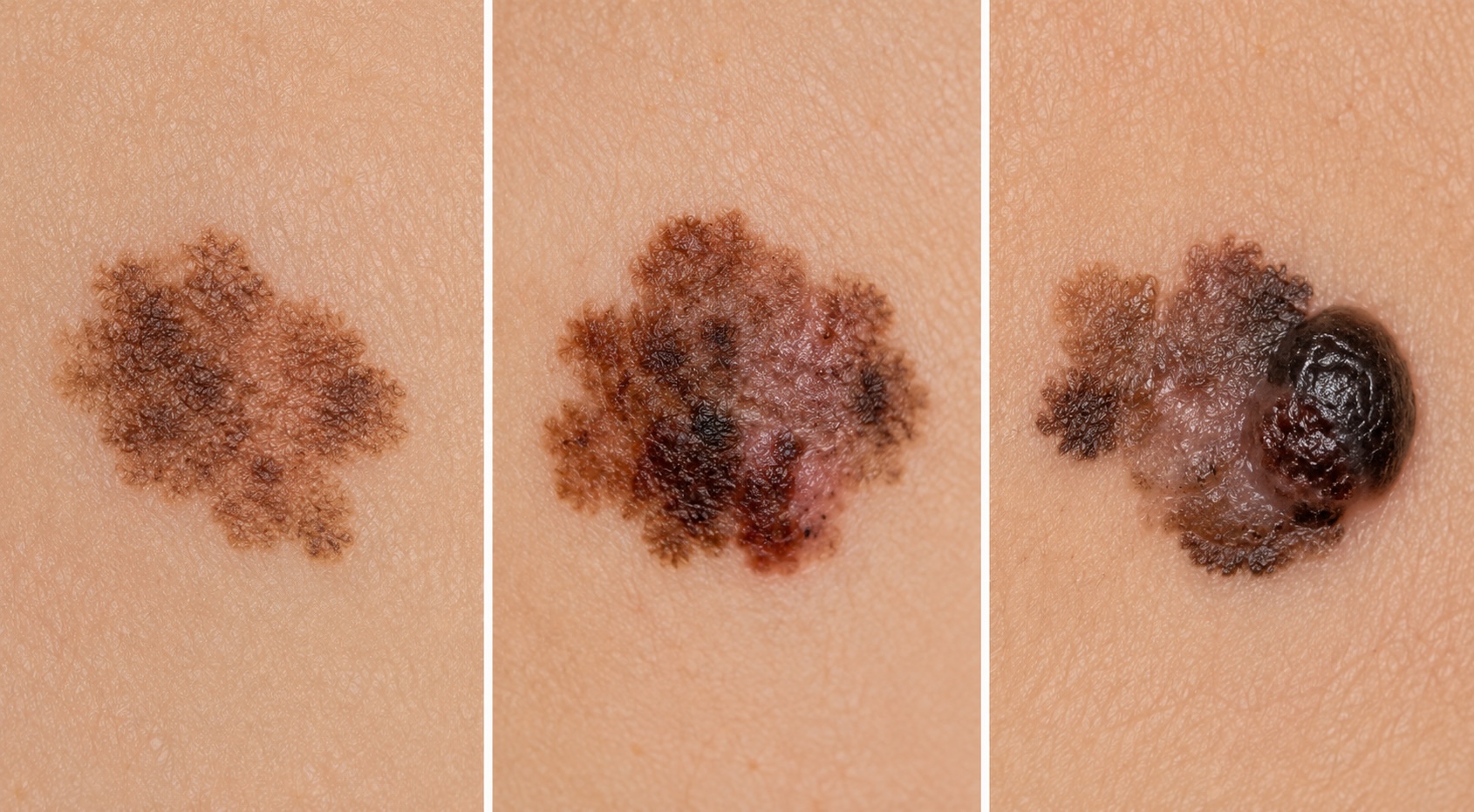
Melanoma classically presents as a new or changing pigmented lesion. The patient (or partner) frequently identifies it before clinical examination. Melanoma can be amelanotic (pink) or hypomelanotic, especially in nodular and desmoplastic variants — a pink, growing lesion in a sun-damaged patient should not be presumed benign without dermoscopy.
The weighted 7-point checklist (Glasgow)
Recommended in NICE NG12 for primary-care triage. Score ≥3 (or any single major feature) → urgent suspected-cancer (2-week-wait) referral.
| Major (2 points each) | Minor (1 point each) |
|---|---|
| Change in size | Diameter ≥7 mm |
| Irregular shape | Inflammation |
| Irregular colour | Oozing or crusting |
| — | Change in sensation |
The ABCDE rule
Asymmetry, Border irregularity, Colour variation, Diameter ≥6 mm, Evolution.
The 'ugly duckling' sign
A lesion morphologically distinct from a patient's other naevi has higher pre-test probability of melanoma than any single ABCDE feature — pattern recognition of intra-person naevus uniformity is a powerful screening tool.


Variants and subtypes
The 2018 WHO classification recognises histogenetic subtypes that reflect different oncogenic pathways and behaviours.
Superficial spreading melanoma (≈60%)
The commonest subtype in fair-skinned populations. Intermittently sun-exposed skin (trunk in men, lower limb in women). Initial radial growth phase as an irregular pigmented macule or thin plaque, with later vertical growth phase. BRAF mutation present in approximately half.
Nodular melanoma (≈15–30%)
Rapid vertical growth without an obvious radial phase. Often dome-shaped, friable, may ulcerate. Higher Breslow at presentation; worse prognosis. Frequently amelanotic.
Lentigo maligna melanoma (≈10%)
Arises in chronically sun-damaged skin (face, dorsal hand) of older patients. Long radial 'lentigo maligna' (in-situ) phase precedes invasion. NRAS, NF1 or c-KIT pathway mutations. See lentigo maligna monograph for in-situ management.

Acral lentiginous melanoma (≈5% UK; up to 30–50% in Fitzpatrick IV–VI)
Palms, soles, subungual. Not UV-driven. KIT mutations common. Diagnostic delay is the rule — index of suspicion for plantar / palmar / subungual pigmentation must remain high in skin of colour. The single greatest equity gap in skin cancer outcome.


Desmoplastic melanoma
Scar-like, often hypomelanotic, predominantly head and neck of older patients. Frequently neurotropic — perineural invasion is a key prognostic feature. SLNB yield is lower than conventional melanoma; nodal recurrence pattern differs. 'Pure' desmoplastic (>90% desmoplastic component) has lower nodal metastatic risk than 'mixed'.
Spitzoid melanoma
Distinct molecular pathway often involving kinase fusions (ALK, ROS1, NTRK1, RET, MET) or HRAS mutations. Diagnostic challenge: distinguishing benign Spitz naevus from atypical Spitz tumour from spitzoid melanoma — see Spitz monograph.
Other rarer variants
- Naevoid melanoma — mimics a benign naevus; easy to miss histologically.
- Mucosal melanoma — see dedicated monograph.
- Uveal melanoma — distinct biology; not covered in detail here.
Dermoscopy
Polarised dermoscopy (10× contact or non-contact) is standard of care in UK pigmented lesion clinics and increases sensitivity and specificity over naked-eye examination — when performed by a trained clinician. See the dermoscopy reference for the comprehensive guide.
Two-step algorithm
- Determine if the lesion is melanocytic or non-melanocytic.
- If melanocytic, apply pattern analysis or a validated algorithm (3-point, 7-point, CASH, Menzies).
Dermoscopic features favouring melanoma
Diagnosis & biopsy
The UK standard for a lesion suspicious for melanoma is a narrow-margin (2 mm) excisional biopsy to the deep subcutis — this allows full Breslow measurement and complete histological assessment. Punch or incisional biopsies are acceptable for large facial or acral lesions where complete excision would be disfiguring or where multiple representative samples are needed.
A superficial shave can transect the deep margin, producing inaccurate Breslow measurement, indeterminate ulceration assessment and upstaging at re-excision. Also avoid laser ablation, cryotherapy or curettage of any suspicious pigmented lesion.
Histopathology — RCPath dataset items
UK histology reports must comply with the RCPath Dataset for histopathological reporting of primary cutaneous malignant melanoma. Core data items include:
- Histogenetic subtype (SSM, nodular, LMM, ALM, desmoplastic).
- Breslow thickness to nearest 0.1 mm.
- Ulceration (present / absent).
- Mitotic rate per mm² (recorded although not in AJCC 8 T-category).
- Microsatellites; lymphovascular invasion; perineural invasion.
- Tumour-infiltrating lymphocytes (TILs); regression.
- Peripheral and deep margins (mm to nearest tumour).
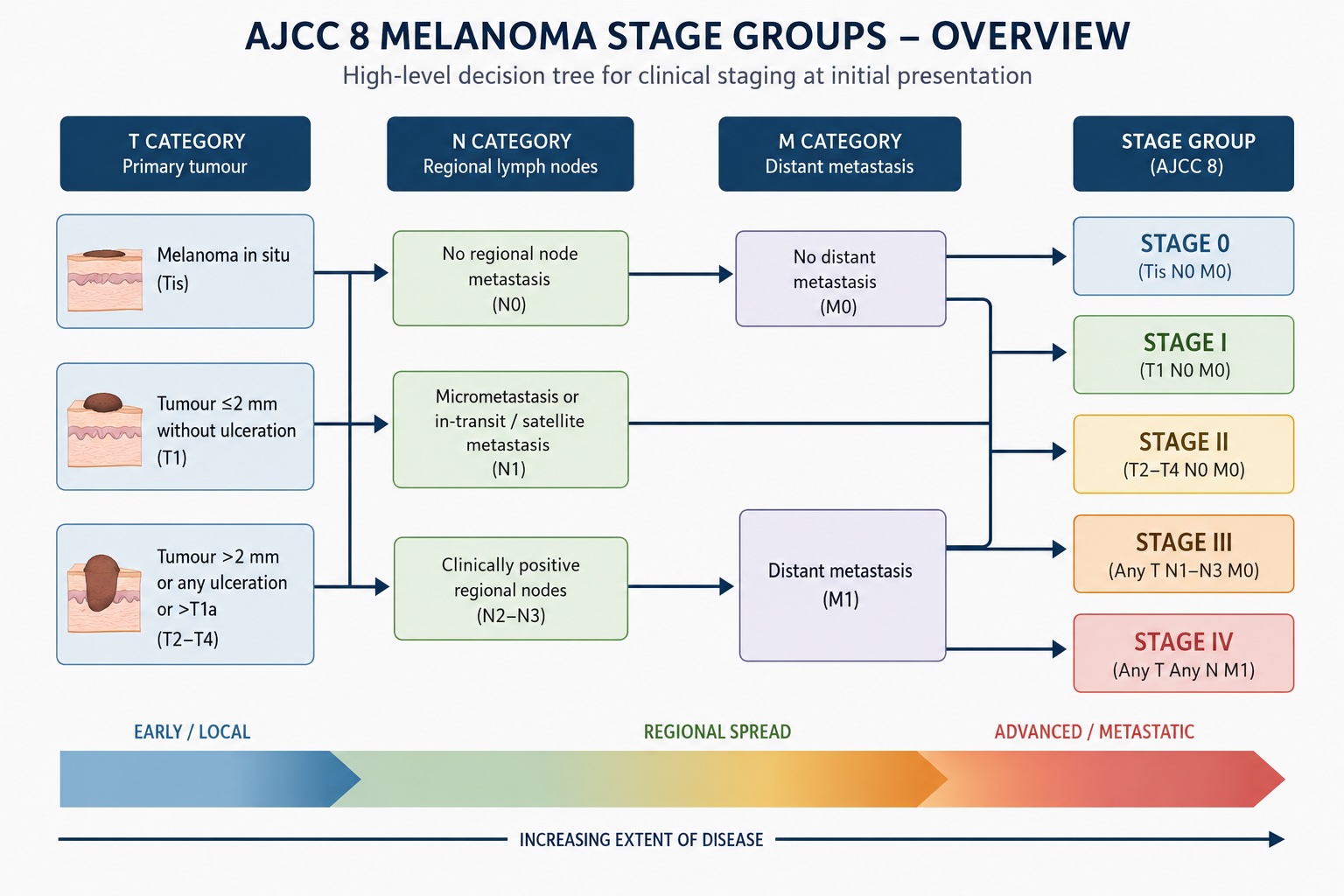
Staging — AJCC 8
UK practice uses AJCC 8th edition TNM staging (effective 2018). Interactive calculator at Tools → Melanoma staging.
T-category
| T | Breslow (mm) | Ulceration |
|---|---|---|
| Tis | In situ | — |
| T1a | <0.8 | No |
| T1b | <0.8 + ulceration, OR 0.8–1.0 ± ulceration | Either |
| T2a / T2b | >1.0–2.0 | No / Yes |
| T3a / T3b | >2.0–4.0 | No / Yes |
| T4a / T4b | >4.0 | No / Yes |
N-category
| N | Definition |
|---|---|
| N0 | No regional metastasis |
| N1a/b | 1 involved node (a = clinically occult / SLN-detected; b = clinically detected) |
| N1c | In-transit / satellite / microsatellite metastases ONLY, with no involved nodes |
| N2a/b | 2–3 involved nodes (a = occult; b = detected) |
| N2c | 1 involved node + in-transit / satellite / microsatellite metastases |
| N3a/b | a = ≥ 4 clinically occult nodes; b = ≥ 4 nodes with at least one clinically detected, or any number of matted nodes |
| N3c | ≥ 2 involved nodes and / or matted nodes, plus in-transit / satellite / microsatellite metastases |
M-category
M0 (no distant metastasis). M1a (skin / soft tissue / non-regional node), M1b (lung), M1c (other visceral), M1d (CNS) — each suffixed with LDH normal (0) / elevated (1).
Investigation by stage
- Stage I–IIA: no routine imaging.
- Stage IIB–IIC: baseline CT NCAP ± brain MRI; discuss adjuvant therapy.
- Stage III: staging CT and MRI brain; PET-CT per MDT.
- Stage IV: CT, MRI brain, LDH; tissue for BRAF and extended NGS panel.
Differential diagnosis
- ●Atypical / dysplastic naevusUsually has clinical and dermoscopic order; uniform colour transitions.
- ●Seborrhoeic keratosisComedo-like openings, milia-like cysts, 'stuck-on' appearance.
- ●Pigmented BCCArborising vessels, blue-grey ovoid nests, leaf-like areas.
- ●Solar lentigo / lentigo simplexLight brown, sharply defined, moth-eaten edge.
- ●Spitz / Reed naevusSymmetrical starburst pattern; in young patients; biopsy if any atypia.
- ●Subungual haematomaAcute trauma, advances distally with nail growth, resolves.
- ●Pyogenic granulomaFriable red papule mimics amelanotic melanoma; biopsy if any concern.
Management by stage
Guideline Wide local excision (WLE) — NICE NG14 margins
| Breslow | Clinical margin |
|---|---|
| Stage 0 / in situ | At least 0.5 cm; consider staged excision or a wider margin for lentigo maligna / head-and-neck sites where subclinical extension is likely |
| Stage I, including T1 and T2a (1.01–2.0 mm without ulceration) | 1 cm |
| Stage II, including T2b (1.01–2.0 mm with ulceration), T3 and T4 | 2 cm; 1 cm only where a 2 cm margin would cause unacceptable disfigurement or morbidity |
Excision is to deep fascia where anatomy permits. Frozen-section margin assessment is not standard for invasive melanoma at trunk and limbs but is used in head-and-neck conservation surgery and lentigo maligna staged excision.
Local MDT Sentinel lymph node biopsy (SLNB)
Do not offer SLNB for stage IA melanoma. NICE NG14 §1.4.3–1.4.4 says to consider SLNB for Breslow 0.8–1.0 mm melanoma with ulceration, lymphovascular invasion or mitotic index of 2/mm² or more, and to consider SLNB for Breslow >1.0 mm melanoma after discussion of benefits, risks and uncertainty. SLNB is staging — it identifies stage III disease that benefits from adjuvant therapy. Completion lymphadenectomy is no longer routine after SLN positivity Trial (MSLT-II) — ultrasound nodal surveillance with adjuvant systemic therapy is the modern standard. CLND remains indicated for macroscopic / palpable / clinically apparent nodal disease, multiple positive SLNs with high extracapsular risk, or where regular ultrasound surveillance is not feasible — the decision sits with the skin-cancer MDT.
Adjuvant systemic therapy
- NICE TA Stage IIB / IIC: pembrolizumab (NICE TA837), 12 months.
- NICE TA Stage III (microscopic, SLNB-detected): adjuvant pembrolizumab (TA766) or nivolumab (TA684); dabrafenib + trametinib for BRAF-mutant stage III (TA544).
- NHS England Stage IIIB–D (macroscopic resectable, age ≥ 12): neoadjuvant followed by adjuvant pembrolizumab — routinely commissioned from 28 April 2026 (URN 2426). Three neoadjuvant doses (3-weekly) precede definitive surgery with therapeutic lymph node dissection within 3–5 weeks of the last dose, followed by adjuvant pembrolizumab to complete 54 weeks total treatment. Off-label use; based on SWOG S1801 (Patel et al, NEJM 2023). Not applicable to microscopic SLNB-detected nodal disease — those patients remain on TA766 / TA684 adjuvant-only.
Locoregionally recurrent / in-transit disease
- Guideline Surgical excision of isolated lesions where feasible.
- Trial Intralesional T-VEC for selected cutaneous / subcutaneous in-transit metastases.
- Local MDT Isolated limb infusion / perfusion in specialist centres.
- NICE TA Systemic immunotherapy for multifocal or unresectable disease.
Metastatic disease
- Trial NICE TA Ipilimumab + nivolumab — longest median OS in multiple phase III trials; higher grade 3–4 irAE rate.
- Trial NICE TA Pembrolizumab or nivolumab monotherapy — well-established, lower toxicity than combination ICI.
- NICE TA Nivolumab + relatlimab (anti-LAG-3) — NICE TA950; emerging role.
- Trial BRAF-mutant: dabrafenib + trametinib; encorafenib + binimetinib — fast responses, limited durability.
- Consensus Brain metastases: stereotactic radiosurgery; combined ipi-nivo has CNS activity.
NICE NG14 (foundation guideline, last updated 27 July 2022). NICE TAs: TA837 (adjuvant pembrolizumab stage IIB/IIC); TA766 (adjuvant pembrolizumab stage III); TA684 (adjuvant nivolumab resected stage III/IV); TA544 (adjuvant dabrafenib + trametinib stage III BRAF V600+); TA384 (nivolumab monotherapy advanced), TA400 (nivolumab + ipilimumab combination); TA396 (dabrafenib + trametinib combination, metastatic); TA562 (encorafenib + binimetinib, metastatic); TA414 (cobimetinib + vemurafenib — not recommended); TA321 (dabrafenib monotherapy, historic); TA410 (T-VEC); TA950 (nivolumab + relatlimab); TA1027 (tebentafusp uveal melanoma, 9 January 2025); TA319 (ipilimumab monotherapy); TA366 (pembrolizumab metastatic). NHS England commissioning policy URN 2426 (28 April 2026): neoadjuvant + adjuvant pembrolizumab for macroscopic resectable stage IIIB–D melanoma, age ≥ 12.
Complications
Locoregional
- Local recurrence (rare with adequate WLE; commonest in desmoplastic and head-and-neck).
- In-transit metastasis (cutaneous / subcutaneous nodules between primary and nodal basin).
- Regional nodal metastasis.
- Lymphoedema after lymphadenectomy.
Distant
- Visceral metastasis (lung, liver, bone, GI, adrenal).
- Brain metastasis — cumulative lifetime involvement up to ~50% (autopsy and long-survival series); symptomatic CNS disease at first presentation in ~20–30%; commoner late event with prolonged survival on ICI.
- Carcinomatous meningitis (rare).
Treatment-related
- Immune-related adverse events (irAEs): pneumonitis, colitis, hepatitis, hypophysitis, thyroid dysfunction, hypoadrenalism, dermatitis, myocarditis. May persist long after ICI discontinuation.
- BRAF/MEK inhibitor toxicity: pyrexia, photosensitivity, second cutaneous neoplasms, ocular events.
- Surgical scar morbidity, sensory change, cosmetic distress.
Follow-up & surveillance
NICE NG14 follow-up is stage-driven. Use the interactive follow-up scheduler for individual timelines and modifiers.
- Stage 0: one clinic advice visit during year 1, then discharge with self-examination advice.
- Stage IA: consider 2 clinic appointments in year 1, then discharge at end of year 1; no routine imaging.
- Stage IB: 2 clinic appointments in year 1, then 1 clinic appointment/year in years 2–5; discharge at end of year 5. Add nodal ultrasound if SLNB was considered but not done.
- Stage IIA: 2 clinic appointments/year in years 1–2, then 1 clinic appointment/year in years 3–5; discharge at end of year 5. Add nodal ultrasound if SLNB was considered but not done.
- Stage IIB: 4 clinic appointments/year in years 1–2, 2 clinic appointments in year 3, then 1/year in years 4–5. Consider whole-body + brain CE-CT surveillance; discharge at end of year 5 if stable.
- Stage IIC: same clinical cadence as IIB, with routine whole-body + brain CE-CT surveillance per NG14; discharge at end of year 5 if stable.
- Stage IIIA–IIIC: if not on adjuvant therapy, 4 clinic appointments/year and 2 whole-body + brain CE-CT scans/year in years 1–3, then 2 clinic appointments/year and 1 scan/year in years 4–5; discharge at end of year 5 if stable. During adjuvant therapy, base follow-up on treatment requirements.
- Stage IIID / resected IV: if not on adjuvant therapy, 4 clinic appointments/year and 4 whole-body + brain CE-CT scans/year in years 1–3, then 2 clinic appointments/year and 2 scans/year in years 4–5; discharge at end of year 5 if stable.
- Unresectable stage III / stage IV: personalised, treatment-led follow-up.
Every visit: full skin examination, regional nodal palpation, systems review for recurrence symptoms, photoprotection counselling, ICI follow-up if applicable.
Special situations
Lentigo maligna of the face
See lentigo maligna monograph. Consider staged excision or Mohs with melanocytic immunostains (MART-1, SOX10) for ill-defined facial lesions; imiquimod is a second-line option.
Acral and subungual melanoma
Longitudinal melanonychia warrants assessment for Hutchinson's sign and early nail-matrix biopsy when concerning. Width >3 mm, irregularity, disruption of parallel lines and triangular shape are dermoscopic red flags. For subungual melanoma in situ, digit-preserving nail-unit excision can be considered in specialist hands. Invasive subungual melanoma should be planned through the melanoma MDT, with oncological clearance taking priority over reconstruction (see hand reconstruction).
Melanoma in pregnancy
Outcomes mirror non-pregnant patients with multidisciplinary input. SLNB feasible — patent blue dye generally avoided (anaphylaxis risk to fetus); technetium alone preferred. Imaging with ionising radiation deferred where possible. Immunotherapy typically deferred until post-partum.
Skin of colour (Fitzpatrick IV–VI)
Acral lentiginous melanoma is proportionally commoner in skin of colour. Outcomes are systematically worse — partly biology, but largely diagnostic delay. The single greatest improvement opportunity is heightened clinician awareness of acral, plantar, palmar and subungual sites in patients with darker skin.
Ocular and mucosal melanoma
Distinct biology and pathways. Refer to ophthalmic oncology / specialist mucosal melanoma services. See mucosal melanoma monograph.
Prognosis
Prognosis is dominated by stage at diagnosis. Approximate AJCC8 5-year melanoma-specific survival (Gershenwald 2017):
| Stage | 5-yr melanoma-specific survival (AJCC8) |
|---|---|
| 0 (in situ) | ~100% |
| IA | ~99% |
| IB | ~97% |
| IIA | ~94% |
| IIB | ~87% |
| IIC | ~82% |
| IIIA | ~93% |
| IIIB | ~83% |
| IIIC | ~69% |
| IIID | ~32% |
| IV | varies widely; markedly improved in the immunotherapy era |
Mitotic rate, ulceration, lymphovascular invasion, microsatellites and gene expression profile refine prognosis within stage groups. Note that stage IIIA survival can exceed that of stage IIB/IIC: low-volume sentinel-node-positive disease (IIIA) carries a better prognosis than a thick, ulcerated node-negative primary (IIC), so the stage groups are not strictly monotonic.
Patient information
This site is for clinicians, but patients often arrive seeking guidance. Direct them to:
- BAD patient information leaflets (melanoma).
- Macmillan Cancer Support.
- Melanoma Focus — UK charity with peer support and resources.
- Their local skin cancer clinical nurse specialist.
References
- NICE NG14. Melanoma: assessment and management. London: NICE; 2015 (last updated 27 July 2022).
- Gershenwald JE et al. Melanoma staging: AJCC 8th edition. CA Cancer J Clin; 2017;67:472–92.
- NICE. Melanoma: assessment and management (NG14). 2022.
- NICE. Suspected cancer (NG12). 2021.
- Royal College of Pathologists. Dataset for histopathological reporting of primary cutaneous malignant melanoma and regional lymph nodes (G125). London: RCPath; February 2019; updated appendices available via the RCPath cancer datasets hub.
- Luke JJ et al. Pembrolizumab in resected stage IIB/IIC melanoma (KEYNOTE-716). Lancet; 2022.
- Tawbi HA et al. Relatlimab + nivolumab vs nivolumab in advanced melanoma (RELATIVITY-047). N Engl J Med; 2022.
- Larkin J et al. Five-year survival with combined nivolumab and ipilimumab. N Engl J Med; 2019;381:1535–46.
- Eggermont AMM et al. Adjuvant pembrolizumab in stage III (KEYNOTE-054). N Engl J Med; 2018.
- Faries MB et al. Completion dissection or observation for sentinel-node metastasis (MSLT-II). N Engl J Med; 2017.
- Bastian BC. The molecular pathology of melanoma. Annu Rev Pathol; 2014;9:239–71.
- Saida T et al. Dermoscopic patterns in acral melanoma. Arch Dermatol; 2004;140:1233–8.
Spot a correction?
If any clinical statement, citation or link on this page needs updating, please email admin@skinoncology.net with the page name, the proposed correction and the supporting source.